The patient is a 49-year-old male that presented to the emergency department with complaints of bilaterally decreased vision, particularly in dim illumination, and eye pain.
His previous medical history was remarkable for hemodialysis due to renal vascular disease and chronic hepatitis due to severe alcoholism; there was also a history of long-standing poor visual acuity in the OD due to a central retinal vein occlusion (CRVO) many years ago.
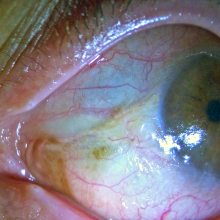
The patient is a 41 years old male who complained of a red, painful, right eye for the past 2 weeks.
Relevant systemic history included asthma and psoriasis. The patient was also morbidly obese.
There was no history of diabetes mellitus or any immune related disease.
He was not a contact lens user.
There was no recollection of ocular trauma.
He denied any relevant ophthalmologic priors, namely ocular surgery, infection or topical eyedrops.
The patient is a 22 year old male that presented as an outpatient to our clinic with complaints of low visual acuity of his left eye.
The patient has a long-standing history of atopy with some bouts of seasonal allergic conjunctivitis.
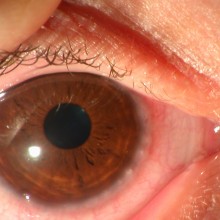
He also suffers from Keratoconus. Assessment of his right eye showed progression to stage 3 in the Amsler-Krumeich classification. He had progressively become intolerant to contact-lens use and presently uses spectacle correction.
The patient is a 6-year-old boy with seasonal conjunctival symptoms (exacerbation in the spring), associated to atopic eczema.
In Spring the eyelids showed mild oedema and blepharitis, the bulbar and tarsal conjunctiva was hyperaemic with papillary reaction, but without the typical giant cobblestone-like papillae.
The cornea showed mild punctate keratopathy and the limbal conjunctiva was thickened and oedematous, with limbal nodules with gelatinous appearance was observed – Trantas’ dots.
The patient is a 28 year old female who was admitted to the emergency department of a different ophthalmology clinic on January 2013 with complaints of burning sensation, photophobia and weeping on
Systemic medical history: asthma, allergic rhinitis, nephrolythiasis
Medication: cetirizine
Ophthalmological medical history;
- Myopia;
- Current vision correction: daily contact lenses (RE: -0,75 D; LE -1,25 D)