
Neurotrophic Ulcer
Authors


The patient is a 41 years old male who complained of a red, painful, right eye for the past 2 weeks.
He had been consulted at a different clinic and was prescribed topical therapy with ofloxacin and cyclopentolate eyedrops.
On November 2013, he was sent to your clinic from a referring hospital with the intent of ruling out the diagnosis of Acanthamoeba keratitis.
Relevant systemic history included asthma and psoriasis. The patient was also morbidly obese.
There was no history of diabetes mellitus or any immune related disease.
He was not a contact lens user.
There was no recollection of ocular trauma.
He denied any relevant ophthalmologic priors, namely ocular surgery, infection or topical eyedrops.
Family history was unremarkable.
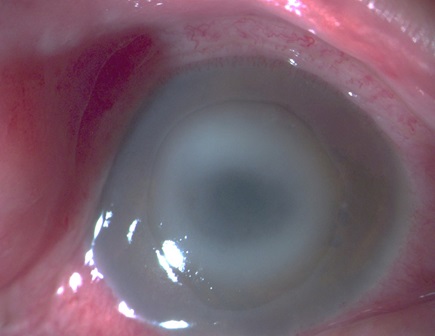
On presentation, visual acuity of the RE was lower than 1/10 and slit lamp examination showed conjunctival redness, a central ulcer with a ring-shaped stromal infiltrate aound it. A small hypopion was observed in the anterior chamber (AC). Best corrected vision of the left eye (LE) was 10/10 and examination of the anterior segment was unremarkable.
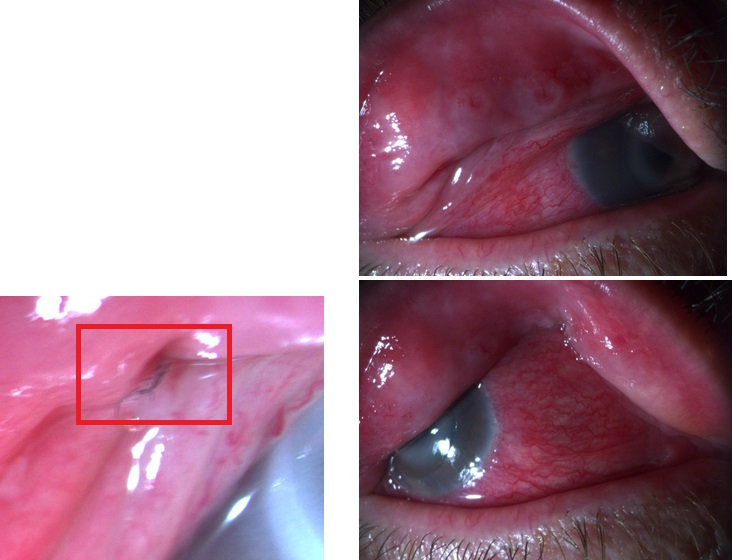
Another striking feature was the presence of a floppy eyelid syndrome, with easy eversion of the superior eyelid. Small fragments of debris, like textile fibers were even found in the conjunctival fornix.
One week after being admitted to our clinic, the patient was feeling better with little or no ocular pain. Corneal ulcer was more circunscribed and with sharply demarcated edges. There was no corneal neovascularization.
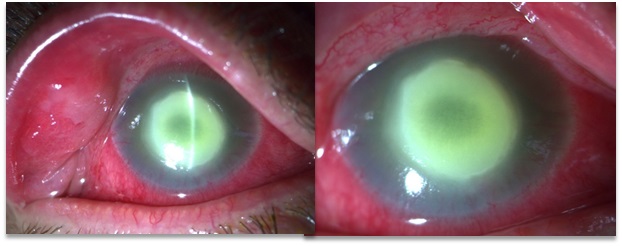
One month after discharge vision had suddenly decreased to hand motion and the patient presented with an enlargement of the ulcer and hypopion.
On January 2014, the patient presented with a stable anterior segment examination, maintaining a deep central corneal ulcer. Corneal neovascularization was now visible.
On the moment the patient finally admitted to topical anesthetic use, the ulcer had increased in size and depth, presenting with rolled but well demarcated edges. Neovascularization were now deeper in the stroma.



Corneal scrapings were sent for culture but came back negative for both bacteria and fungi.
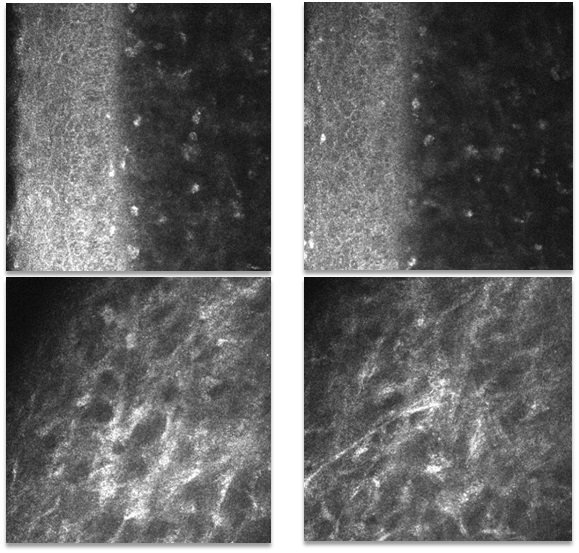
Confocal microscopy was performed, showing epithelial disorganization and basal membrane disruption. Intermediate stroma showed some fibrosis and rare activated keratocytes. Noticeably, no fungal hyphae and Acanthamoeba cysts or trophozoytes were observed.
Due to indolent rate of improvement with appropriate therapy, a polymerase chain reaction (PCR) analysis was requested to confirm the diagnosis of Acanthamoeba keratitis. The result eventually came back negative.
Almost 2 months after the first observation, and after being emphatically confronted with that hypothesis on numerous occasions... the patient finally breaks down and admits to long term abusive use of topical Oxybuprocaine
