Topography Guided PRK in a Penetrating keratoplasty
Authors


Man aged 38, diagnosed with bilateral keratoconus (KC) 21 years ago.
In 1996 he was submitted to a penetrating keratoplasty (PK) in the left eye (LE), due to a corneal central leukoma and best corrected visual acuity (BCVA) of less than 1/10 (Snellen), without complications. One year after LE PK, he had a clear graft, without neovascularization, uncorrected visual acuity (UCVA) of 5/10 and BCVA of 8/10 with -1.00 (+1.50 x 130º). BCVA improved to 10/10 with +1.00 (-3.25 x 40º) in the second year post-op.
In 2000, he had an uneventful PK in the right eye (RE) due to a corneal central leukoma. Two years later, the graft was clear and BCVA was 10/10 with (+2.50 x 120º).
In 2015, 19 years after LE PK and 15 years after RE PK, he was observed in the cornea consultation, where he had RE VA of 10/10 with +2.00 (-5.00 x 15º) and LE VA of 12/10 with -0.75 (-2.00 x 25º); both grafts were transparent and the remainder ophthalmic examination was otherwise unremarkable.
There is a history of asthmatic bronchitis, treated with Salbutamol SOS.
External examination and ocular motility were normal.
At the last visit, 15 years after PK in the RE, visual acuities were 10/10 with +2,00 (-5,00 x 15º)in the RE and 12/10 with -0,75 (-2,00 x 25º) in the LE.
Biomicroscopy showed clear grafts without neovascularization, deep anterior chambers, reactive pupils and transparent lens in both eyes.
Fundoscopy revealed C/D 0,5-0,6 in both eyes.
Intraocular pressure was 14 mmHg bilaterally.
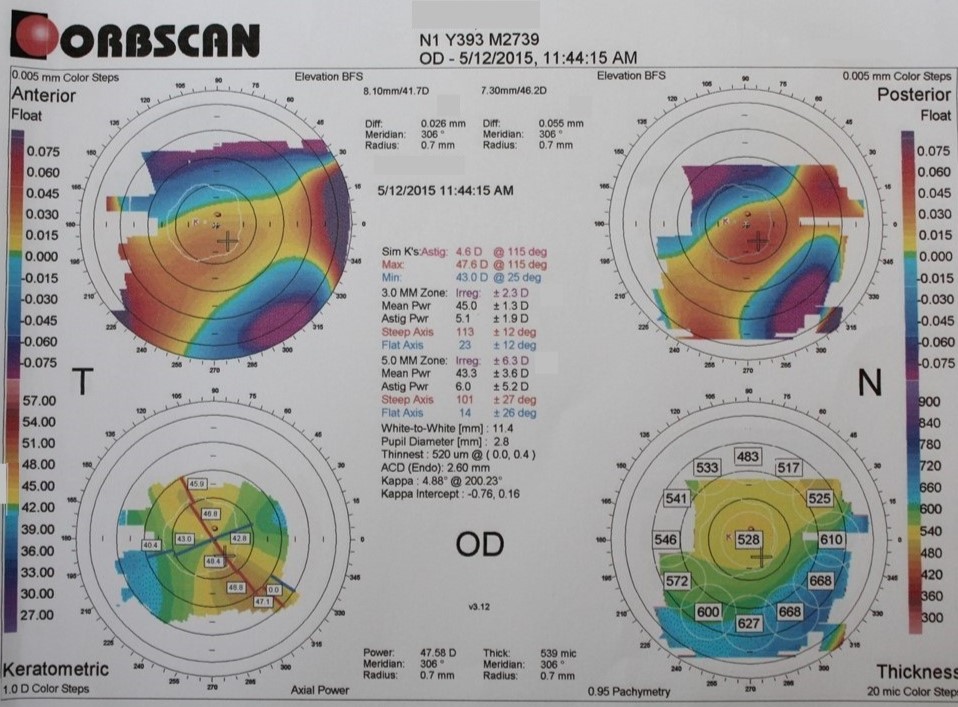
Corneal topography (Orbscan) revealed accentuated corneal astigmatism in the RE.
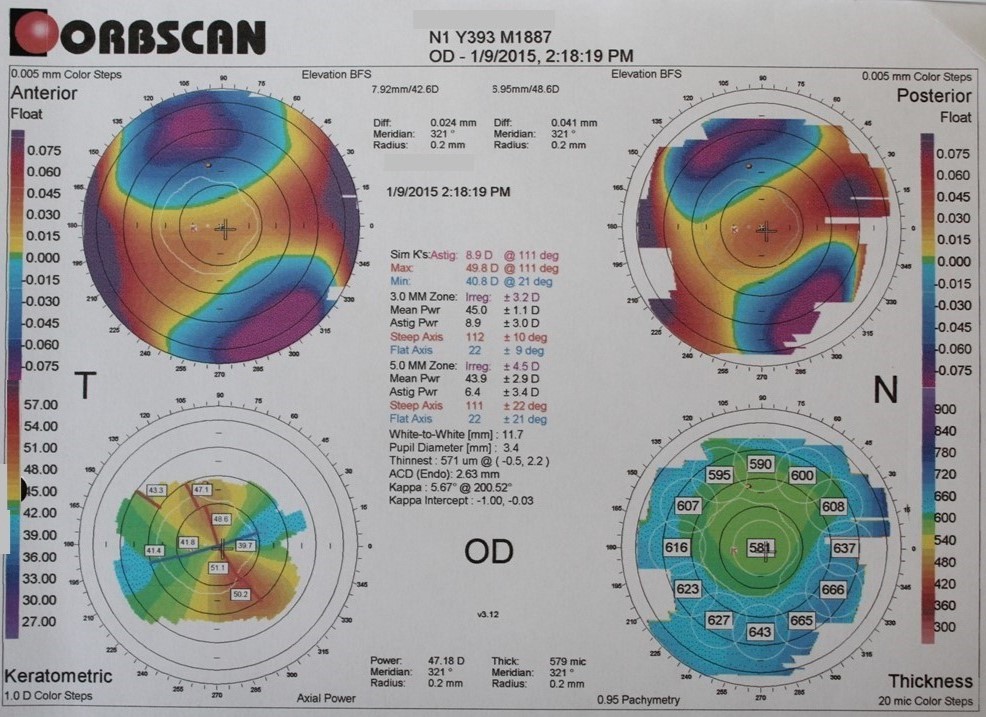
High ammetropia after PK.
The patient underwent topography guided photorefractive keratectomy (PRK) with mitomycin C 30 seconds in the RE. Post-operative medication included broad-spectrum topical antibiotic, fluorometholone 4id (tapered over 1 month) and lubrication.
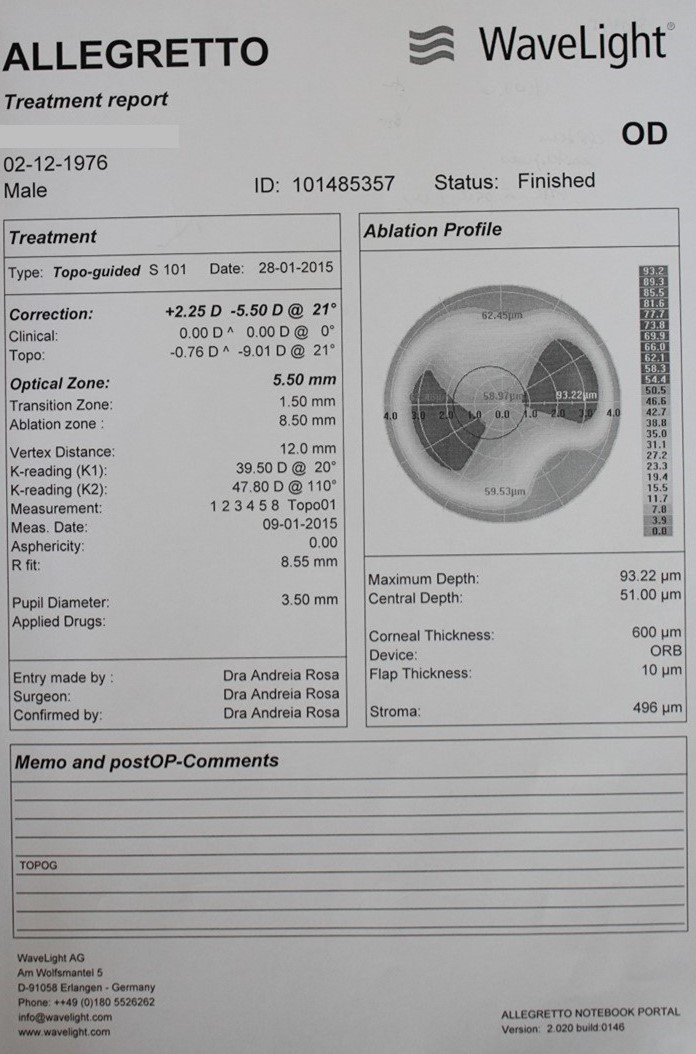
There was a significant improvement of the refractive error after topography guided PRK, from a preoperative refractive error of +2.00 (-5.00 x 15º), to +0.75 (-1.50 x 20º) at 3 months post-op.